

Introduction to Cervicogenic Headaches (CGH)
In our clinical practice, we frequently see patients who suffer from persistent headaches that don’t respond to typical migraine treatments. Often, the culprit isn’t in the head at all, but in the neck. This is known as a Cervicogenic Headache (CGH).
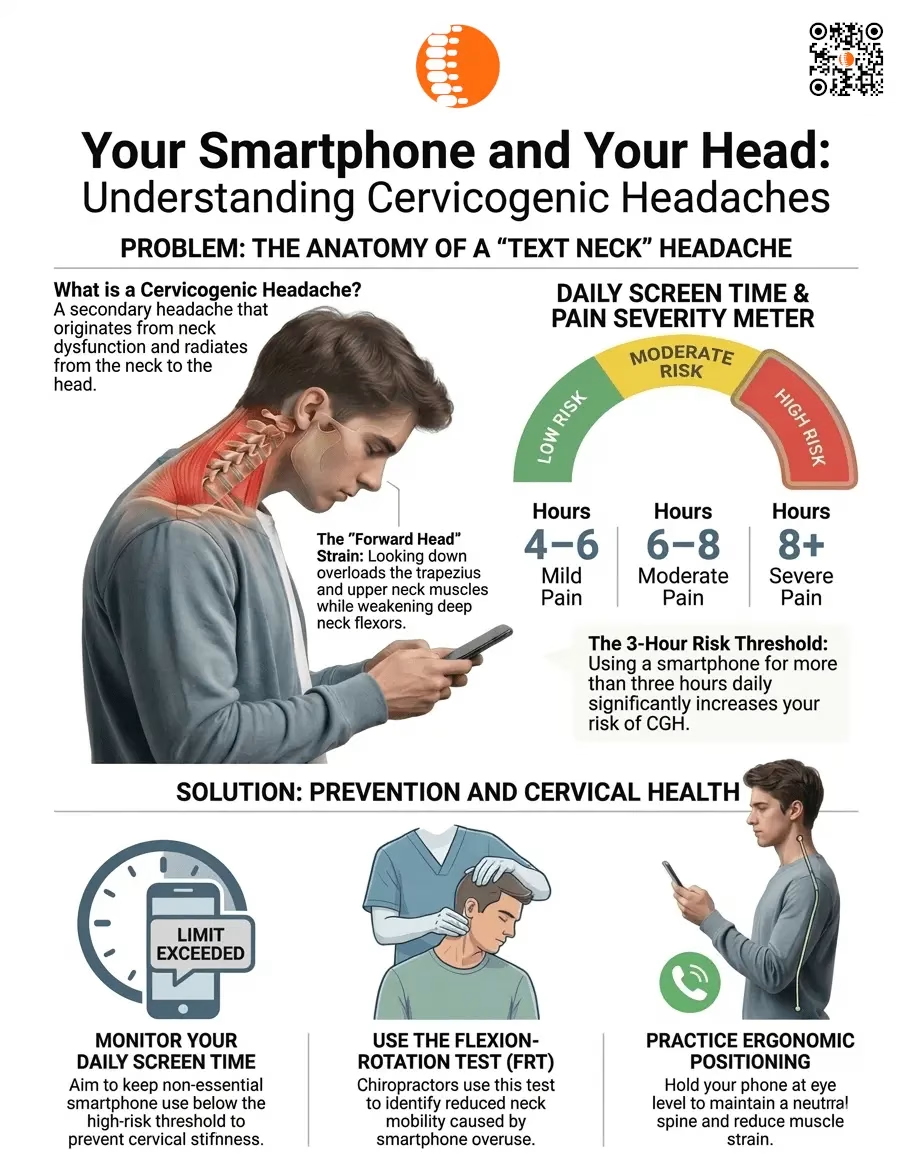
We classify CGH as a “secondary headache,” meaning the pain is a symptom of an underlying physical issue in the cervical spine (your neck). Specifically, this involves dysfunction in the upper cervical vertebrae (C1, C2, and C3), the C2–C3 intervertebral discs, and the upper synovial joints. When these structures are strained—often by the way we hold our devices—they send distress signals to the brain.
Why Neck Issues Feel Like Head Pain
You might wonder why a neck problem feels like a forehead or behind-the-eye ache. This happens because of the trigeminocervical nucleus. Think of this as a major “electrical junction box” in your nervous system where pain signals from your upper neck and the sensory nerves of your face and head converge. Because these signals overlap, your brain can become “cross-wired,” misinterpreting a neck problem as pain in your head.
Identifying the Symptoms
When you come into my clinic, I look for specific “red flags” that distinguish CGH from other conditions. These include:
- Radiation Pattern: Pain that usually starts at the base of the skull or neck and travels toward the back (occipital) or front (frontal) of the head.
- Non-Throbbing Pain: Unlike migraines, which often pulse, CGH is typically a steady, dull ache.
- Movement Triggers: Pain that worsens when you turn your head, hold a specific posture for too long, or when a therapist applies pressure to the “trigger points” in your neck.
- Restricted Mobility: A feeling of “stiffness” or a literal inability to turn your head as far as you used to.
Cervicogenic headaches are frequently confused with migraines or cluster headaches. Furthermore, they are often linked to cervical spondylosis (age related “grey hair” of the spine). If your headaches are consistently tied to neck stiffness, it is important to assess the spine rather than just treating the head pain.
The Smartphone Link: Understanding Your Risk
In our modern lifestyle, the biggest threat to your cervical health is likely in your pocket. Our research highlights a “3-Hour Threshold”: accumulating more than three hours of smartphone use per day significantly increases your risk of developing CGH.
It is important to remember that these hours are cumulative. Small increments of scrolling throughout the day add up to a high-risk zone. As screen time increases, the intensity of the pain typically follows a predictable pattern:
| Daily Screen Time | Typical Pain Severity (Pain rated out of 10) |
| 4–6 Hours | Mild Pain (0-3) |
| 6–8 Hours | Moderate Pain (4-7) |
| More than 8 Hours | Severe Pain (8-10) |
A Note on Gender: While women are statistically more likely to suffer from CGH globally, our latest data shows that among smartphone users, males often report a higher mean pain intensity (1.93 on the scale) compared to females (1.59). Regardless of your gender, your risk increases the longer you stay glued to the screen.
The Mechanics of “Forward Head Posture”
When you lean your head forward to look at a screenyou are essentially doubling or tripling the weight your neck muscles must support. This leads to a specific type of muscle imbalance:
- Superficial Stiffness: Muscles like the levator scapulae, sternocleidomastoid (SCM), and upper trapezius become chronically tight and stiff as they struggle to hold your head up.
- Deep Weakness: The deep neck flexors, the essential “core” muscles of your neck that provide stability, become weak and inhibited from disuse.
What this means for your recovery: This imbalance creates a cycle of spinal strain and compromised motor control, eventually leading to the functional limitations and headaches you are experiencing.
How Healthcare Providers Diagnose CGH
To confirm that your headaches are originating from your neck, we use two primary clinical tools:
- Cervical Flexion-Rotation Test (FRT): This is the gold standard for CGH diagnosis. Your therapist will gently move your neck into specific angles to check mobility at the C1–C2 level. This test has a 92% sensitivity rate, making it highly accurate for identifying neck-related headaches. In a recent study of 175 students, 136 participants (over 77%) tested positive on the FRT, showcasing how common this issue has become.
- Numeric Pain Rating Scale (NPRS): We use this 0–10 scale to track your progress and understand the severity of your symptoms during daily activities.
Practical Strategies for Prevention and Management
Recovery involves more than just “sitting up straight.” It requires a dedicated approach to how you interact with technology:
- Monitor Accumulated Time: Use “Screen Time” apps to track your daily usage. Aim to keep your total phone use below the 3-hour mark whenever possible.
- Raise the Device, Not the Neck: Bring your phone up to eye level. It is much easier to move your arms than it is to repair a strained cervical spine.
- Correct the Imbalance: Focus on exercises that strengthen the deep neck flexors while stretching the stiff superficial muscles like the trapezius.
- Seek Targeted Intervention: Consult a physical therapist for manual therapy. Specialized techniques, such as C1-C2 mobilization, can restore lost movement and provide immediate relief from referred head pain.
Summary Checklist for Spinal Health
Use this checklist daily to protect your neck and reduce the frequency of your headaches:
- [ ] Limit cumulative smartphone use to under 3 hours per day.
- [ ] Perform an eye-level check: Is my device at eye level, or am I looking down?
- [ ] Reset your posture every 15 minutes by aligning your ears over your shoulders.
- [ ] Discuss manual therapy and C1-C2 mobilization with your physical therapist.
- [ ] Strengthen deep stabilizers and stretch the superficial neck muscles daily.
For Further Reading (References)
The evidence provided in this guide is based on recent clinical research. You are encouraged to share these findings with your primary care provider: